A | B | C | D | E | F | G | H | CH | I | J | K | L | M | N | O | P | Q | R | S | T | U | V | W | X | Y | Z | 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9
| Temporomandibular joint dysfunction | |
|---|---|
| Other names | Temporomandibular joint dysfunction syndrome, temporomandibular disorder, others[1] |
 | |
| Temporomandibular joint | |
| Specialty | Oral and maxillofacial surgery, Oral medicine |
Temporomandibular joint dysfunction (TMD, TMJD) is an umbrella term covering pain and dysfunction of the muscles of mastication (the muscles that move the jaw) and the temporomandibular joints (the joints which connect the mandible to the skull). The most important feature is pain, followed by restricted mandibular movement,[2] and noises from the temporomandibular joints (TMJ) during jaw movement. Although TMD is not life-threatening, it can be detrimental to quality of life;[3] this is because the symptoms can become chronic and difficult to manage.
In this article, the term temporomandibular disorder is taken to mean any disorder that affects the temporomandibular joint, and temporomandibular joint dysfunction (here also abbreviated to TMD) is taken to mean symptomatic (e.g. pain, limitation of movement, clicking) dysfunction of the temporomandibular joint. However, there is no single, globally accepted term or definition[4] concerning this topic.
TMDs have a range of causes and often co-occur with a number of overlapping medical conditions, including headaches, fibromyalgia, back pain, and irritable bowel.[5] However, these factors are poorly understood,[6] and there is disagreement as to their relative importance. There are many treatments available,[7] although there is a general lack of evidence for any treatment in TMD, and no widely accepted treatment protocol. Common treatments include provision of occlusal splints, psychosocial interventions like cognitive behavioral therapy, physical therapy, and pain medication or others. Most sources agree that no irreversible treatment should be carried out for TMD.[8]
About 20% to 30% of the adult population are affected to some degree.[7] Usually people affected by TMD are between 20 and 40 years of age,[3] and it is more common in females than males.[9] TMD is the second most frequent cause of orofacial pain after dental pain (i.e. toothache).[10]
Classification
|
TMD is considered by some to be one of the 4 major symptom complexes in chronic orofacial pain, along with burning mouth syndrome, atypical facial pain and atypical odontalgia.[12] TMD has been considered as a type of musculoskeletal,[13] neuromuscular,[14] or rheumatological disorder.[13] It has also been called a functional pain syndrome,[6] and a psychogenic disorder.[15] [16] It is hypothesized that there is a great deal of similarity between TMD and other pain syndromes like fibromyalgia, irritable bowel syndrome, interstitial cystitis, headache, chronic lower back pain and chronic neck pain.
Definitions and terminology
Frequently, TMD has been treated as a single syndrome, but the prevailing modern view is that TMD is a cluster of related disorders with many common features.[13] Indeed, some have suggested that, in the future, the term 'TMD' may be discarded as the different causes are fully identified and separated into different conditions.[15] Sometimes, "temporomandibular joint dysfunction" is described as the most common form of temporomandibular disorder,[17] whereas many other sources use the term 'temporomandibular disorder' synonymously, or instead of the term 'temporomandibular joint dysfunction'. In turn, the term 'temporomandibular disorder' is defined as "musculoskeletal disorders affecting the temporomandibular joints and their associated musculature. It is a collective term which represents a diverse group of pathologies involving the temporomandibular joint, the muscles of mastication, or both".[2] Another definition of temporomandibular disorders is "a group of conditions with similar signs and symptoms that affect the temporomandibular joints, the muscles of mastication, or both."[18] 'Temporomandibular disorder' is a term that creates confusion since it refers to a group of similarly symptomatic conditions, whilst many sources use the term temporomandibular disorders as a vague description, rather than a specific syndrome, and refer to any condition which may affect the temporomandibular joints (see table). The temporomandibular joint is susceptible to a huge range of diseases, some rarer than others, and there is no implication that all of these will cause any symptoms or limitation in function at all.[citation needed]
The preferred terms in medical publications is to an extent influenced by geographic location. For example, in the United Kingdom, the term 'pain dysfunction syndrome' is in common use.[17] In the United States, the term 'temporomandibular disorder' is generally favored. The American Academy of Orofacial Pain uses 'temporomandibular disorder', whilst the National Institute of Dental and Craniofacial Research uses 'temporomandibular joint disorder'.[4] A more complete list of synonyms for this topic is extensive, with some being more commonly used than others. In addition to those already mentioned, examples include 'temporomandibular joint pain dysfunction syndrome', 'temporomandibular pain dysfunction syndrome', 'temporomandibular joint syndrome', 'temporomandibular dysfunction syndrome', 'temporomandibular dysfunction', 'temporomandibular disorder', 'temporomandibular syndrome', 'facial arthromyalgia', 'myofacial pain dysfunction syndrome', 'craniomandibular dysfunction' (CMD), 'myofacial pain dysfunction', 'masticatory myalgia', 'mandibular dysfunction', and 'Costen's syndrome'.
The lack of standardization in terms is not restricted to medical papers. Notable internationally recognized sources vary in both their preferred term, and their offered definition. For example:
"Temporomandibular Pain and Dysfunction Syndrome – Aching in the muscles of mastication, sometimes with an occasional brief severe pain on chewing, often associated with restricted jaw movement and clicking or popping sounds." (Classification of Chronic Pain, International Association for the Study of Pain).[19]
"Headache or facial pain attributed to temporomandibular joint disorder." (International Classification of Headache Disorders 2nd edition (ICHD-2), International Headache Society).[20]
"Temporomandibular joint-pain-dysfunction syndrome" listed in turn under "Temporomandibular joint disorders" (International Classification of Diseases 10th revision, World Health Organization).[21]
By cause and symptoms
It has been suggested that TMD may develop following physical trauma, particularly whiplash injury, although the evidence for this is not conclusive. This type of TMD is sometimes termed "posttraumatic TMD" (pTMD) to distinguish it from TMD of unknown cause, sometimes termed "idiopathic TMD" (iTMD).[13] Sometimes muscle-related (myogenous) TMD (also termed myogenous TMD, or TMD secondary to myofascial pain and dysfunction) is distinguished from joint-related TMD (also termed arthogenous TMD, or TMD secondary to true articular disease), based upon whether the muscles of mastication or the TMJs themselves are predominantly involved. This classification, which effectively divides TMD into 2 syndromes, is followed by the American Academy of Orofacial Pain.[4] However, since most people with TMD could be placed into both of these groups, which makes a single diagnosis difficult when this classification is used. The Research Diagnostic Criteria (RDC/TMD) allows for multiple diagnoses in an attempt to overcome the problems with other classifications. RDC/TMD considers temporomandibular disorders in 2 axes; axis I is the physical aspects, and axis II involves assessment of psychological status, mandibular function and TMD-related psychosocial disability.[4] Axis I is further divided into 3 general groups. Group I are muscle disorders, group II are disc displacements and group III are joint disorders,[10] although it is common for people with TMD to fit into more than one of these groups.
By duration
Sometimes distinction is made between acute TMD, where symptoms last for less than 3 months, and chronic TMD, where symptoms last for more than 3 months.[2] Not much is known about acute TMD since these individuals do not typically attend in secondary care (hospital).[2]
Signs and symptoms
Signs and symptoms of temporomandibular joint disorder vary in their presentation. The symptoms will usually involve more than one of the various components of the masticatory system, muscles, nerves, tendons, ligaments, bones, connective tissue, or the teeth.[22]
The three classically described, cardinal signs and symptoms of TMD are:[10][23]
- Pain and tenderness on palpation in the muscles of mastication, or of the joint itself (preauricular pain – pain felt just in front of the ear). Pain is the defining feature of TMD and is usually aggravated by manipulation or function,[2] such as when chewing, clenching,[11] or yawning, and is often worse upon waking. The character of the pain is usually dull or aching, poorly localized,[6] and intermittent, although it can sometimes be constant. The pain is more usually unilateral (located on one side) rather than bilateral.[19] It is rarely severe.[24]
- Limited range of mandibular movement,[2] which may cause difficulty eating or even talking. There may be locking of the jaw, or stiffness in the jaw muscles and the joints, especially present upon waking.[18] There may also be incoordination, asymmetry or deviation of mandibular movement.[2]
- Noises from the joint during mandibular movement, which may be intermittent.[17] Joint noises may be described as clicking,[2] popping,[19] or crepitus (grating).[18]
TMJ dysfunction is commonly associated with symptoms affecting cervical spine dysfunction and altered head and cervical spine posture.[25]
Other signs and symptoms have also been described, although these are less common and less significant than the cardinal signs and symptoms listed above. Examples include:
- Headache (possibly),[17] e.g. pain in the occipital region (the back of the head), or the forehead;[11] or other types of facial pain including migraine,[22] tension headache,[22] or myofascial pain.[22]
- Pain elsewhere, such as the teeth[11] or neck.[9]
- Diminished auditory acuity (hearing loss).[22]
- Tinnitus (occasionally).[18]
- Dizziness.[9]
- Sensation of malocclusion (feeling that the teeth do not meet together properly).[19]
Causes
TMD is a symptom complex (i.e. a group of symptoms occurring together and characterizing a particular disease), which is thought to be caused by multiple, poorly understood factors,[17][26][6] but the exact etiology is unknown.[27] There are factors which appear to predispose to TMD (genetic, hormonal, anatomical), factors which may precipitate it (trauma, occlusal changes, parafunction), and also factors which may prolong it (stress and again parafunction).[18] Overall, two hypotheses have dominated research into the causes of TMD, namely a psychosocial model and a theory of occlusal dysharmony.[27] Interest in occlusal factors as a causative factor in TMD was especially widespread in the past, and the theory has since fallen out of favor and become controversial due to lack of evidence.
Disc displacement
In people with TMD, it has been shown that the lower head of lateral pterygoid contracts during mouth closing (when it should relax), and is often tender to palpation. To theorize upon this observation, some have suggested that due to a tear in the back of the joint capsule, the articular disc may be displaced forwards (anterior disc displacement), stopping the upper head of lateral pterygoid from acting to stabilize the disc as it would do normally. As a biologic compensatory mechanism, the lower head tries to fill this role, hence the abnormal muscle activity during mouth closure. There is some evidence that anterior disc displacement is present in a proportion of TMD cases. Anterior disc displacement with reduction refers to abnormal forward movement of the disc during opening which reduces upon closing. Anterior disc displacement without reduction refers to an abnormal forward, bunched-up position of the articular disc which does not reduce. In this latter scenario, the disc is not intermediary between the condyle and the articular fossa as it should be, and hence the articular surfaces of the bones themselves are exposed to a greater degree of wear (which may predispose to osteoarthritis in later life).[26]
Degenerative joint disease
The general term "degenerative joint disease" refers to arthritis (both osteoarthritis and rheumatoid arthritis) and arthrosis. The term arthrosis may cause confusion since in the specialized TMD literature it means something slightly different from in the wider medical literature. In medicine generally, arthrosis can be a nonspecific term for a joint, any disease of a joint (or specifically degenerative joint disease), and is also used as a synonym for osteoarthritis.[28] In the specialized literature that has evolved around TMD research, arthrosis is differentiated from arthritis by the presence of low and no inflammation respectively.[6] Both are however equally degenerative.[6] The TMJs are sometimes described as one of the most used joints in the body. Over time, either with normal use or with parafunctional use of the joint, wear and degeneration can occur, termed osteoarthritis. Rheumatoid arthritis, an autoimmune joint disease, can also affect the TMJs. Degenerative joint diseases may lead to defects in the shape of the tissues of the joint, limitation of function (e.g. restricted mandibular movements), and joint pain.[6]
Psychosocial factors
Emotional stress (anxiety, depression, anger) may increase pain by causing autonomic, visceral and skeletal activity and by reduced inhibition via the descending pathways of the limbic system. The interactions of these biological systems have been described as a vicious "anxiety-pain-tension" cycle which is thought to be frequently involved in TMD. Put simply, stress and anxiety cause grinding of teeth and sustained muscular contraction in the face. This produces pain which causes further anxiety which in turn causes prolonged muscular spasm at trigger points, vasoconstriction, ischemia and release of pain mediators. The pain discourages use of the masticatory system (a similar phenomenon in other chronic pain conditions is termed "fear avoidance" behavior), which leads to reduced muscle flexibility, tone, strength and endurance. This manifests as limited mouth opening and a sensation that the teeth are not fitting properly.[12]
Persons with TMD have a higher prevalence of psychological disorders than people without TMD.[29] People with TMD have been shown to have higher levels of anxiety, depression, somatization and sleep deprivation, and these could be considered important risk factors for the development of TMD.[26][29] In the 6 months before the onset, 50–70% of people with TMD report experiencing stressful life events (e.g. involving work, money, health or relationship loss). It has been postulated that such events induce anxiety and cause increased jaw muscle activity. Muscular hyperactivity has also been shown in people with TMD whilst taking examinations or watching horror films.[26]
Others argue that a link between muscular hyperactivity and TMD has not been convincingly demonstrated, and that emotional distress may be more of a consequence of pain rather than a cause.[27]
Bruxism
Bruxism is an oral parafunctional activity where there is excessive clenching and grinding of the teeth. It can occur during sleep or whilst awake. The cause of bruxism itself is not completely understood, but psychosocial factors appear to be implicated in awake bruxism and dopaminergic dysfunction and other central nervous system mechanisms may be involved in sleep bruxism. If TMD pain and limitation of mandibular movement are greatest upon waking, and then slowly resolve throughout the day, this may indicate sleep bruxism. Conversely, awake bruxism tends to cause symptoms that slowly get worse throughout the day, and there may be no pain at all upon waking.
The relationship of bruxism with TMD is debated. Many suggest that sleep bruxism can be a causative or contributory factor to pain symptoms in TMD.[26][27][30][31] Indeed, the symptoms of TMD overlap with those of bruxism.[32] Others suggest that there is no strong association between TMD and bruxism.[24] A systematic review investigating the possible relationship concluded that when self-reported bruxism is used to diagnose bruxism, there is a positive association with TMD pain, and when more strict diagnostic criteria for bruxism are used, the association with TMD symptoms is much lower.[33] Self-reported bruxism is probably a poor method of identifying bruxism.[31] There are also very many people who grind their teeth and who do not develop TMD.[18] Bruxism and other parafunctional activities may play a role in perpetuating symptoms in some cases.[34]
Other parafunctional habits such as pen chewing, lip and cheek biting (which may manifest as morsicatio buccarum or linea alba), are also suggested to contribute to the development of TMD.[26] Other parafunctional activities might include jaw thrusting, excessive gum chewing, nail biting and eating very hard foods.
Trauma
Trauma, both micro and macrotrauma, is sometimes identified as a possible cause of TMD; however, the evidence for this is not strong.[24] Prolonged mouth opening (hyper-extension) is also suggested as a possible cause. It is thought that this leads to microtrauma and subsequent muscular hyperactivity. This may occur during dental treatment, with oral intubation whilst under a general anesthetic, during singing or wind instrument practice (really these can be thought of as parafunctional activities).[26] Damage may be incurred during violent yawning, laughing, road traffic accidents, sports injuries, interpersonal violence, or during dental treatment,[24] (such as tooth extraction).[26]
It has been proposed that a link exists between whiplash injuries (sudden neck hyper-extension usually occurring in road traffic accidents), and the development of TMD. This has been termed "post-traumatic TMD", to separate it from "idiopathic TMD".[13] Despite multiple studies having been performed over the years, the cumulative evidence has been described as conflicting, with moderate evidence that TMD can occasionally follow whiplash injury.[13] The research that suggests a link appears to demonstrate a low to moderate incidence of TMD following whiplash injury, and that pTMD has a poorer response to treatment than TMD which has not developed in relation to trauma.[13]
Occlusal factors
Occlusal factors as an etiologic factor in TMD is a controversial topic.[26] Abnormalities of occlusion (problems with the bite) are often blamed for TMD but there is no evidence that these factors are involved.[24] Occlusal abnormalities are incredibly common, and most people with occlusal abnormalities do not have TMD.[35] Although occlusal features may affect observed electrical activity in masticatory muscles,[36] there are no statistically significant differences in the number of occlusal abnormalities in people with TMD and in people without TMD.[26] There is also no evidence for a causal link between orthodontic treatment and TMD.[26] The modern, mainstream view is that the vast majority of people with TMD, occlusal factors are not related.[18] Theories of occlusal factors in TMD are largely of historical interest. A causal relationship between occlusal factors and TMD was championed by Ramfjord in the 1960s.[15] A small minority of dentists continue to prescribe occlusal adjustments in the belief that this will prevent or treat TMD despite the existence of systematic reviews of the subject which state that there is no evidence for such practices,[37] and the vast majority of opinion being that no irreversible treatment should be carried out in TMD (see Occlusal adjustment).
Genetic factors
TMD does not obviously run in families like a genetic disease[dubious – discuss]. It has been suggested that a genetic predisposition for developing TMD (and chronic pain syndromes generally) could exist. This has been postulated to be explained by variations of the gene which codes for the enzyme catechol-O-methyl transferase (COMT) which may produce 3 different phenotypes with regards pain sensitivity. COMT (together with monoamine oxidase) is involved in breaking down catecholamines (e.g. dopamine, epinephrine, and norepinephrine). The variation of the COMT gene which produces less of this enzyme is associated with a high sensitivity to pain. Females with this variation, are at 2–3 times greater risk of developing TMD than females without this variant. However this theory is controversial since there is conflicting evidence.[6]
Hormonal factors
Since females are more often affected by TMD than males, the female sex hormone estrogen has been suggested to be involved.[6] The results of one study suggested that the periods of highest pain in TMD can be correlated with rapid periods of change in the circulating estrogen level. Low estrogen was also correlated to higher pain.[15] In the menstrual cycle, estrogen levels fluctuate rapidly during ovulation, and also rapidly increases just before menstruation and rapidly decreases during menstruation. Post-menopausal females who are treated with hormone replacement therapy are more likely to develop TMD, or may experience an exacerbation if they already had TMD. Several possible mechanisms by which estrogen might be involved in TMD symptoms have been proposed. Estrogen may play a role in modulating joint inflammation, nociceptive neurons in the trigeminal nerve, muscle reflexes to pain and μ-opioid receptors.[6]
Possible associations
TMD has been suggested to be associated with other conditions or factors, with varying degrees of evidence and some more commonly than others. 75% of people with TMD qualify for a fibromyalgia diagnosis and, conversely, 18% of people with fibromyalgia met diagnostic criteria for TMD.[16] A possible link between many of these chronic pain conditions has been hypothesized to be due to shared pathophysiological mechanisms, and they have been collectively termed "central sensitivity syndromes",[16] although other apparent associations cannot be explained in this manner. Recently a plethora of research has substantiated a causal relationship between TMD and Obstructive Sleep Apnea (OSA). Severe TMD restricts oral airway opening, and can result in a retrognathic posture that results in glossal blockage of the oropharynx as the tongue relaxes in sleep. This mechanism is exacerbated by alcohol consumption, as well as other chemicals that result in reduced myotonic status of the oropharynx.
- Obstructive sleep apnea.[38][39]
- Headache.[16]
- Chronic neck pain.[16]
- Chronic back pain.[15]
- Systemic joint laxity.[18]
- Rheumatoid arthritis.[18]
- Irritable bowel syndrome.[16]
- Interstitial cystitis.[16]
- Regular scuba diving.[26][40]
Pathophysiology



Anatomy and physiology
Temporomandibular joints
The temporomandibular joints are the dual articulation of the mandible with the skull. Each TMJ is classed as a "ginglymoarthrodial" joint since it is both a ginglymus (hinging joint) and an arthrodial (sliding) joint,[41] and involves the condylar process of the mandible below, and the articular fossa (or glenoid fossa) of the temporal bone above. Between these articular surfaces is the articular disc (or meniscus), which is a biconcave, transversely oval disc composed of dense fibrous connective tissue. Each TMJ is covered by a fibrous capsule. There are tight fibers connecting the mandible to the disc, and loose fibers which connect the disc to the temporal bone, meaning there are in effect 2 joint capsules, creating an upper joint space and a lower joint space, with the articular disc in between. The synovial membrane of the TMJ lines the inside of the fibrous capsule apart from the articular surfaces and the disc. This membrane secretes synovial fluid, which is both a lubricant to fill the joint spaces, and a means to convey nutrients to the tissues inside the joint. Behind the disc is loose vascular tissue termed the "bilaminar region" which serves as a posterior attachment for the disc and also fills with blood to fill the space created when the head of the condyle translates down the articular eminence.[42] Due to its concave shape, sometimes the articular disc is described as having an anterior band, intermediate zone and a posterior band.[43] When the mouth is opened, the initial movement of the mandibular condyle is rotational, and this involves mainly the lower joint space, and when the mouth is opened further, the movement of the condyle is translational, involving mainly the upper joint space.[44] This translation movement is achieved by the condylar head sliding down the articular eminence, which constitutes the front border of the articular fossa.[35] The function of the articular eminence is to limit the forwards movement of the condyle.[35] The ligament directly associated with the TMJ is the temporomandibular ligament, also termed the lateral ligament, which really is a thickening of the lateral aspect of the fibrous capsule.[35] The stylomandibular ligament and the sphenomandibular ligament are not directly associated with the joint capsule. Together, these ligaments act to restrict the extreme movements of the joint.[45]
Muscles of mastication
The muscles of mastication are paired on each side and work together to produce the movements of the mandible. The main muscles involved are the masseter, temporalis and medial and lateral pterygoid muscles.
-
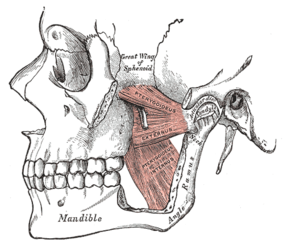 Left medial and lateral pterygoid muscles
Left medial and lateral pterygoid muscles -
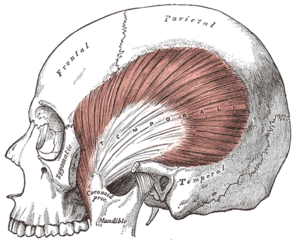 Left temporalis muscle
Left temporalis muscle -
 Left masseter muscle (red highlight)
Left masseter muscle (red highlight)


.png)
They can be thought of in terms of the directions they move the mandible, with most being involved in more than one type of movement due to the variation in the orientation of muscle fibers within some of these muscles.
- Protrusion – Lateral and medial pterygoid.
- Retraction – Posterior fibers of temporalis (and the digastric and geniohyoid muscles to a lesser extent).
- Elevation – Anterior and middle fibers of temporalis, the superficial and deep fibers of masseter and the medial pterygoid.[42]
- Lateral movements – Medial and lateral pterygoid (the ipsilateral temporalis and the pterygoid muscles of the contralateral side pull the mandible to the ipsilateral side).[35]
Each lateral pterygoid muscle is composed of 2 heads, the upper or superior head and the lower or inferior head. The lower head originates from the lateral surface of the lateral pterygoid plate and inserts at a depression on the neck of mandibular condyle, just below the articular surface, termed the pterygoid fovea. The upper head originates from the infratemporal surface and the infratemporal crest of the greater wing of the sphenoid bone. The upper head also inserts at the fovea, but a part may be attached directly to the joint capsule and to the anterior and medial borders of the articular disc.[42] The 2 parts of lateral pterygoid have different actions. The lower head contracts during mouth opening, and the upper head contracts during mouth closing. The function of the lower head is to steady the articular disc as it moves back with the condyle into the articular fossa. It is relaxed during mouth closure.[26]
Mechanisms of symptoms
Joint noises
Noises from the TMJs are a symptom of dysfunction of these joints. The sounds commonly produced by TMD are usually described as a "click" or a "pop" when a single sound is heard and as "crepitation" or "crepitus" when there are multiple, grating, rough sounds. Most joint sounds are due to internal derangement of the joint, which is instability or abnormal position of the articular disc.[46] Clicking often accompanies either jaw opening or closing, and usually occurs towards the end of the movement. The noise indicates that the articular disc has suddenly moved to and from a temporarily displaced position (disk displacement with reduction) to allow completion of a phase of movement of the mandible.[26][27] If the disc displaces and does not reduce (move back into position) this may be associated with locking. Clicking alone is not diagnostic of TMD since it is present in high proportion of the general population, mostly in people who have no pain.[26] Crepitus often indicates arthritic changes in the joint, and may occur at any time during mandibular movement, especially lateral movements.[26] Perforation of the disc may also cause crepitus.[35] Due to the proximity of the TMJ to the ear canal, joint noises are perceived to be much louder to the individual than to others. Often people with TMD are surprised that what sounds to them like very loud noises cannot be heard at all by others next to them. However, it is occasionally possible for loud joint noises to be easily heard by others in some cases and this can be a source of embarrassment e.g. when eating in company.
Pain
Pain symptoms in TMD can be thought of as originating from the joint (arthralgia), or from the muscles (myofascial), or both. There is a poor correlation between TMD pain severity and evidence of tissue pathology.[6]
Generally, degenerative joint changes are associated with greater pain.
Myofascial pain
Pain originating from the muscles of mastication as a result of abnormal muscular function or hyperactivity. The muscular pain is frequently, but not always, associated with daytime clenching or nocturnal bruxism.[47]
Limitation of mandibular movementedit
The jaw deviates to the affected side during opening,[19] and restricted mouth opening usually signifies that both TMJs are involved, but severe trismus rarely occurs. If the greatest reduction in movement occurs upon waking then this may indicate that there is concomitant sleep bruxism. In other cases the limitation in movement gets worse throughout the day.[26]
The jaw may lock entirely.[26]
Limitation of mandibular movement itself may lead to further problems involving the TMJs and the muscles of mastication. Changes in the synovial membrane may lead to a reduction in lubrication of the joint and contribute to degenerative joint changes.[48] The muscles become weak, and fibrosis may occur. All these factors may lead to a further limitation of jaw movement and increase in pain.[48]
Degenerative joint disease, such as osteoarthritis or organic degeneration of the articular surfaces, recurrent fibrous or bony ankylosis, developmental abnormality, or pathologic lesions within the TMJ. Myofascial pain syndrome.[medical citation needed]
Referred TMD painedit
Sometimes TMD pain can radiate or be referred from its cause (i.e. the TMJ or the muscles of mastication) and be felt as headaches, earache or toothache.[11]
Due to the proximity of the ear to the temporomandibular joint, TMJ pain can often be confused with ear pain.[22] The pain may be referred in around half of all patients and experienced as otalgia (earache).[49] Conversely, TMD is an important possible cause of secondary otalgia. Treatment of TMD may then significantly reduce symptoms of otalgia and tinnitus, as well as atypical facial pain.[50] Despite some of these findings, some researchers question whether TMJD therapy can reduce symptoms in the ear, and there is currently an ongoing debate to settle the controversy.[22]
Diagnosisedit
|
Group I: muscle disorders Ia. Myofascial pain:
Ib. Myofascial pain with limited opening:
Group II: disc displacements IIa. Disc displacement with reduction:
IIb. Disc displacement without reduction with limited opening:
IIc. Disc displacement without reduction, without limited opening:
Group III: arthralgia, osteoarthritis, osteoarthrosis IIIa. Arthralgia:
IIIb. Osteoarthritis of the TMJ:
IIIc. Osteoarthrosis of the TMJ:
|

Pain is the most common reason for people with TMD to seek medical advice.[2] Joint noises may require auscultation with a stethoscope to detect.[19] Clicks of the joint may also be palpated, over the joint itself in the preauricular region, or via a finger inserted in the external acoustic meatus,[18] which lies directly behind the TMJ. The differential diagnosis is with degenerative joint disease (e.g. osteoarthritis), rheumatoid arthritis, temporal arteritis, otitis media, parotitis, mandibular osteomyelitis, Eagle syndrome, trigeminal neuralgia,[medical citation needed] oromandibular dystonia,[medical citation needed] deafferentation pains, and psychogenic pain.[19]
Diagnostic criteriaedit
Various diagnostic systems have been described. Some consider the Research Diagnostic Criteria method the gold standard.[18] Abbreviated to "RDC/TMD", this was first introduced in 1992 by Dworkin and LeResche in an attempt to classify temporomandibular disorders by etiology and apply universal standards for research into TMD.[52] This method involves 2 diagnostic axes, namely axis I, the physical diagnosis, and axis II, the psychologic diagnosis.[18] Axis I contains 3 different groups which can occur in combinations of 2 or all 3 groups,[18] (see table).
McNeill 1997 described TMD diagnostic criteria as follows:[2]
- Pain in muscles of mastication, the TMJ, or the periauricular area (around the ear), which is usually made worse by manipulation or function.
- Asymmetric mandibular movement with or without clicking.
- Limitation of mandibular movements.
- Pain present for a minimum of 3 months.
The International Headache Society's diagnostic criteria for "headache or facial pain attributed to temporomandibular joint disorder" is similar to the above:[20]
- A. Recurrent pain in one or more regions of the head or face fulfilling criteria C and D
- B. X-ray, MRI or bone scintigraphy demonstrate TMJ disorder
- C. Evidence that pain can be attributed to the TMJ disorder, based on at least one of the following:
- pain is precipitated by jaw movements or chewing of hard or tough food
- reduced range of or irregular jaw opening
- noise from one or both TMJs during jaw movements
- tenderness of the joint capsule(s) of one or both TMJs
- D. Headache resolves within 3 months, and does not recur, after successful treatment of the TMJ disorder
Medical imagingedit
The advantages brought about by diagnostic imaging mainly lie within diagnosing TMD of articular origin. Additional benefits of imaging the TMJ are as follows:[53]
- Assess the integrity of anatomical structures in suspicion of disorders
- Staging the extent of any pathology
- Monitoring and staging the progress of disease
- Determining the effects of treatment
When clinical examination alone is unable to bring sufficient detail to ascertain the state of the TMJ, imaging methods can act as an adjuvant to clinical examination in the diagnosis of TMD.[53]
Plain radiographyedit
This method of imaging allows the visualisation of the joint's mineralised areas, therefore excluding the cartilage and soft tissues.[53] A disadvantage of plain radiography is that images are prone to superimposition from surrounding anatomical structures, thereby complicating radiographic interpretation.[53] It was concluded that there is no evidence to support the use of plain radiography in the diagnosis of joint erosions and osteophytes.[54] It is reasonable to conclude that plain film can only be used to diagnose extensive lesions.[54]
Panoramic tomographyedit
The distortion brought about by panoramic imaging decreases its overall reliability. Data concluded from a systematic review showed that only extensive erosions and large osteophytes can be detected by panoramic imaging.[54]
Computerised tomography (CT)edit
Studies have shown that tomography of the TMJ provided supplementary information that supersedes what is obtainable from clinical examination alone.[55] However, the issues lies in the fact that it is impossible to determine whether certain patient groups would benefit more or less from a radiographic examination.[56]
Zdroj:https://en.wikipedia.org?pojem=Temporomandibular_joint_dysfunction
>Text je dostupný pod licencí Creative Commons Uveďte autora – Zachovejte licenci, případně za dalších podmínek. Podrobnosti naleznete na stránce Podmínky užití.
Text je dostupný za podmienok Creative
Commons Attribution/Share-Alike License 3.0 Unported; prípadne za ďalších
podmienok.
Podrobnejšie informácie nájdete na stránke Podmienky
použitia.

